
Chapter 16 - Violence and Tragedies
Family Functions and Dysfunctions
Families are functional at some levels and simultaneously dysfunctional at others. No two families are exactly alike, and very few families experience blissful, ideal family experiences. Think about it, how could a family be ideal when its members are mortals? It can't. Even in the history and myths of ancient civilizations, families had dysfunctions. For example, Father Abraham's polygamous family had two sons, Ishmael (first-born) and Isaac (second-born). Ishmael and Isaac could not live together because their family broke up as a result of their mothers not getting along (their descendants still hold traditional enmity over these issues). Royal histories are filled with sibling rivalry, incestuous relationships, and violence.
The Roman lore of its founding history includes the fight between two adult brothers over what would eventually become Rome, wherein the twin boys were nearly drowned by their uncle (Google "Romulus and Remus" to be surprised at who these twins' stepmother proved to be). Ancient Greek mythology is also full of family feuding and fighting and discord (Google "Prometheus," "Hercules," "Oedipus," and "Narcissus"). And these characters were assumed to be gods! Again, all modern families have functions and dysfunctions.
Family Functions are the tasks and goals that support and sustain the family. Dysfunctions are failures in the family to accomplish these tasks and goals. Functions are intended. Dysfunctions are typically unintended. For example, family members do not intend to establish poor communication patterns, invisible sexual boundaries (incest), or economic hardships. The basic family functions that are intended include economic cooperation, control of sexuality, socializing children, identity and social status, and social and emotional need fulfillment.

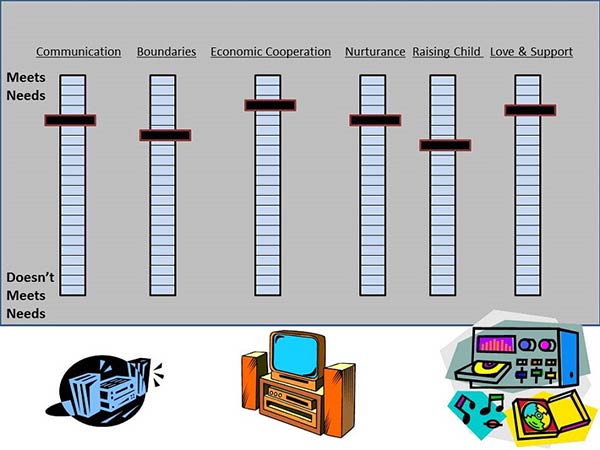
Figures 1 and 2 show diagrams of how family functions and dysfunctions can be compared to an equalizer on a stereo system. In Figure 1 this family meets the needs of communication, boundaries that are in place and maintained, economic cooperation, nurturance through relationships, raising the child/children, and offering love and support to other family members. Some families meet family members' needs better than others. These are often referred to as being High-Resource Families. There are other families that meet some needs well and other needs poorly.
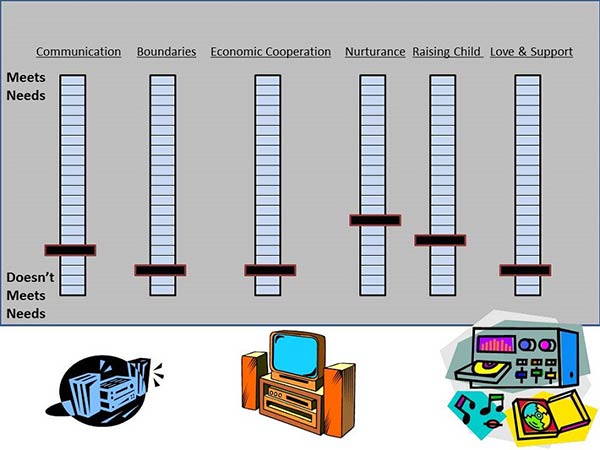
Figure 2 shows a family that meets most needs poorly. These are called Low-Resource Families. This family fails to meet the needs of communication, boundaries that are in place and maintained, economic cooperation, nurturance through relationships, raising the child/children, and offering love and support to other family members. This looks like a hopeless situation, but with voluntary efforts at seeking help or even involuntary efforts (state intervention), more resources could be attained and the family may improve its functionality.
Figure 1. How Families Are Functional or Dysfunctional in Meeting Specific Needs: High-Resource Family
Family dysfunctions can be handed down from generation to generation, with few family members aware that something is wrong in the family system. I know of a 62-year-old man who shared with me in private that he was the first in a long line of family members who did NOT sexually abuse other family members. "I broke the chain of abuse," he declared. His father would not acknowledge the abuse, much less talk to him about his having broken the chain.
Figure 2. How Families Are Functional or Dysfunctional in Meeting Specific Needs: Low-Resource Family
A Core issue to address is about Safety for: Children, Women, and Men in U.S. Society
A Set of United Nations guidelines was pass in 1989 that has guided how many countries structure their civil and criminal laws to best protect the well-being of children living within their borders. The Convention on the Rights of the Child states:
“States Parties shall take all appropriate legislative, administrative, social and educational measures to protect the child from all forms of physical or mental violence, injury or abuse, neglect or negligent treatment, maltreatment or exploitation, including sexual abuse, while in the care of parent(s), legal guardian(s) or any other person who has the care of the child (see OHCHR at UN retrieved 8 August 2020 from SOURCE ).”
Although these rights are not universally binding nor enforced (for example with criminal penalties when violated), they are well-designed, multi-nationally developed, and ideal guidelines designed to protect children. Protecting children from 9 forms of violence is worth investing governmental funds in both social, educational, and I would add criminal justice laws in behalf of all children in the world (and specifically in the United States). All of these safeguards could be applied to the rights of women and men.
Figure 3 shows a diagram of safety for children, women, and men as of the year 2020. It is safe to say that most children, most women, and most men are safe, but none of us are safe from any trauma all the time. The United States Population as of 1 July 2019 was estimated to be about 328.239.523-people strong (Census, 2019). As you look at Figure 3, you can see that no matter how old you are, each of us is at some level of risk (24 hours per day, 7 days per week) of suffering at least one of these unsafe trauma caused by another person against us. Thank goodness the risks are not indicating that something would happen each day to each person. But if we are alive (and we are) we are at risks of one or more of these happening at some point in our lives. Among the 52+ million U.S. elderly national and local police agencies deal with each of these issues every year. With the adults who make up the largest portion of the country, police also deal with such acts of violence and mistreatment(see NCVS 2018 data). The school age and pre-school age are at even more risk than the older members of society since they are less able to protect themselves for perpetrators. So, what about that radioactive isotope symbol about to crash into the column in Figure3; what is or are ACES? We will not discuss every one of these traumas listed in Figure 3. We will focus on a few.
Figure 3. Diagram of Safety for Children, Women, and Men as of the year 2020.*
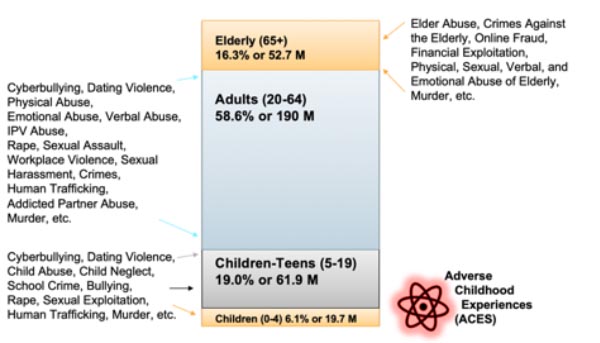
*Proportions of Age and Sex collected from U.S. Census on 8 Aug. 2020 from Quick Facts and derived from Census Table 1. Population by Age and Sex: 2019 downloaded 8 Aug 2020 from SOURCE
Aces are Adverse Childhood Experiences which include 1 or more traumatic childhood experiences which have happened in a child’s life prior to turning 18 (see ACES). The CDC includes these childhood traumatic events: experiencing violence, abuse, or neglect; witnessing violence in the home or community; having a family member attempt suicide or die by suicide; childhood instability due to parental mental health problems, addictions, or involvement with law enforcement agencies (being arrested). The CDC states about 61% of adults surveyed in 25 states have had at least 1 and some have had far more. After decades of very rigorous scientific studies the CDC stated that “ACEs are linked to chronic health problems, mental illness, and substance misuse in adulthood. ACEs can also negatively impact education and job opportunities. However, ACEs can be prevented.” (CDC 2019 Centers for Disease Control and Prevention (2019). Preventing Adverse Childhood Experiences: Leveraging the Best Available Evidence. Atlanta, GA: National Center for Injury Prevention and Control, Centers for Disease Control and Prevention. Retrieved 8 August 2020 from SOURCE ). Why use a radioactive isotope symbol to portray ACES? If a person is ever exposed to any form of radiation, that radiation has the potential to damage their body immediately and the resulting consequences will cause added suffering for the rest of that person’s life. The more radiation exposure the more damage and suffering. Likewise, the more ACES a person suffers the more damage and lifelong suffering for that person’s entire life (a life which could even be shorter than if no ACES were experienced).
Violence and Abuse
Family Abuse is the physical, sexual, or emotional maltreatment or harm of another family member. It is unethical, immoral, and illegal. If you were like me, and you grew up in an abusive home, please accept the fact that it was not your fault. Abuse is perpetrated by powerful people on less powerful people. Young children should be protected by older family members from predators and non-family members who could cause harm. If you were not protected, or worse, if you were preyed upon by someone who was supposed to protect you, then it is their fault, not yours!
You may have heard that there is a chain of abuse passed from parent to child to grandchild. That may be true, but not if you don't want it to be in your case. Some estimates place it at 1 in 3 sexually abused children grow up to be abusers. Many abuse survivors are meticulous about marrying non-abusers and about over-protecting their children from potential abusers. Based on my professional and private research in the area of surviving abuse, I'd urge you to seek professional help and support for dealing with your childhood traumas. There are numerous free resources. Again, it is not your fault, but healing is your responsibility. It is not enough to simply ignore or deny the abuse. That would be like trying to heal from a 2-inch wood sliver that is lodged in your leg by simply ignoring it.
Sexual abuse is a particularly sinister form of abuse. The American Academy of Child and Adolescent Psychiatry reported that 80,000 cases of child sexual abuse are reported each year in the U.S., with many more cases unreported. They list possible symptoms:
"Sexually abused children may also develop the following: unusual interest in or avoidance of all things of a sexual nature, sleep problems or nightmares, depression or withdrawal from friends or family, seductiveness, statements that their bodies are dirty or damaged, or fear that there is something wrong with them in the genital area, refusal to go to school, delinquency/conduct problems, secretiveness, aspects of sexual molestation in drawings, games, fantasies, unusual aggressiveness, or suicidal behavior." (Retrieved June 14, 2014 AM Acad. Of Child & Adol. Psychiatry SOURCE and SOURCE )Nowhere in this document (or any professional document based on treating survivors) does it blame the victim. Yet it does urge adult and child survivors of abuse and their family members to seek out professional help and support.
One way to approach child abuse awareness and prevention as a parent or grandparent is to teach your child a simple rule about their safety. Many of the available programs on child sexual abuse prevention use the "No Touch" style of this rule. I teach my students to teach their children this simple rule -- no one should touch you where your shirt and shorts cover your body! That is your "no touch zone." Don't let anyone touch your chest, tummy, hips, buttocks, between the legs, or thighs. If anyone does, then scream "stop!" And tell your mom or dad, teacher, or other trusted adult. There is a useful PDF file free from the uS Center for Disease Control "Preventing Child Sexual Abuse Within Youth-serving Organizations: Getting Started on Policies and Procedures on preventing sexual abuse" provided by the Centers for Disease Control.
Now you also have to teach them the difference in a family hug and unwanted, inappropriate touch. But teach it! That's where most parents fail in this regard. They don't want to talk about it (especially if their own wounds are unhealed), and they rarely bring it up. Of special concern to me as the father of 5 sons is the increasing trend of adult-female-to-teen-male sexual abuse trends. The news regularly broadcast stories of teachers, teacher's aids, coaches, and mothers of the teen's friends who are seducing and raping teen boys. Most states do not prosecute these abuse cases as they would a male-adult-to-female-minor case (often called forcible or statutory rape). Both boys and girls should be protected from sexual misconduct by adults with the threat of felony charges for the adult perpetrator.
Recent U.S. data indicates that there were about 700,000 U.S. children abused or neglected in 2018. Taken together there were official efforts on the party of state welfare authorities to ensure that 3.5 million children were actually safe and from those efforts, 1.9 million received prevention services. Of them, 1,770 children died. Also concerning was the overall trend of various forms of alleged abuse that was investigated including: (Child sexual abuse (65^); Physical abuse (21%); Neglect (8%); drug endangerment from their caregivers/parents (3%); and some others). About 7 percent witnessed adult violence that year. These troubling data are not unique. Many annual reports show similar rates of maltreatment that have to be investigated or stopped (see Factsheet from the National Children’s Alliance, National Statistics on Child Abuses 2018 retrieved 8 August 2020 from SOURCE).
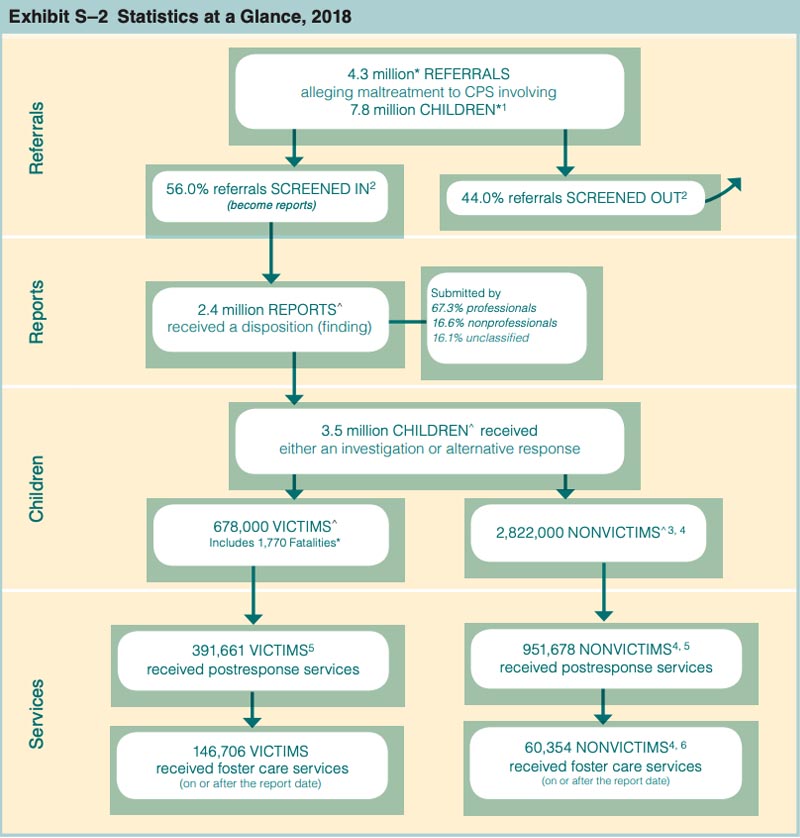
Figure 4 shows child maltreatment data indicating 4.3 million referrals (allegations) that included a total of 7.8 million potentially maltreated US children. Of these, 2.4 million were responded to by Child Protective Services. Of them 678,000 were found to be victims and 1,770 children had died. As the flow chart continues you see near the bottom of the page that 207,060 received various forms of foster care services (add 146,706 + 60,354). The remainder of the cases were kept on file, dismissed, or managed as described in the boxes above. Many US children are maltreated every year, whether legal or criminal intervention resulted from the investigation or not. Many more or maltreated and the allegations go unreported.
This same report noted a general 2018 pattern of higher child abuse and neglect allegations for the youngest children with the rate/1,000 being at 26.7 (Newborns); 11.8 (age 1); 11 (age 2); 10.3 (age 3); 9.8 (age 4); 9.7 (age 5); and so forth declining each year without exceptions until reaching 3.7 for age 17 (See Exhibit 3-D Victims by Age, 2018; page 20). The rates for boys (8.7) and girls (9.6) were very similar. All together when consider the nature of the child’s family member accused of the abuses, 91.7 percent were of victims were maltreated by their own parents. Overall, 60.8 percent were found to have been neglected; 10.7 percent physically abused; and 7.0 percent sexually abused. Of those who lost their lives boys had a fatality rate of 2.87/100,000 and girls had a rate of 2.19/100,000. This 262-page report is free as a pdf download, has comprehensive state by state data and a variety of other state-specific information sources from SOURCE (also a variety of annual reports from 1995-2018 can be downloaded from SOURCE).
Figure 4. US Flow Chart with Statistics on Child Maltreatment through the Social Service Systems 2018*
In families, abuse may also be perpetrated by adults against adults. When violence occurs between adult spouses and partners, it is often called intimate partner violence, or IPV. The CDC provides a useful definition: "In the context of this document, intimate partner violence (IPV) is defined as actual or threatened physical, sexual, psychological, emotional, or stalking abuse by an intimate partner. An intimate partner can be a current or former spouse or non-marital partner, such as a boyfriend, girlfriend, or dating partner" (see CDC 2017 Niolon, P. H., Kearns, M., Dills, J., Rambo, K., Irving, S., Armstead, T., & Gilbert, L. (2017). Preventing Intimate Partner Violence Across the Lifespan: A Technical Package of Programs, Policies, and Practices. Atlanta, GA: National Center for Injury Prevention and Control, Centers for Disease Control and Prevention retrieved 8 August 2020 from SOURCE).
This CDC report also provides an executive summary of known risks including:
“IPV affects millions of people in the United States each year. Data from the National Intimate Partner and Sexual Violence Survey (NISVS) indicate that nearly 1 in 4 adult women (23%) and approximately 1 in 7 men (14%) in the U.S. report having experienced severe physical violence (e.g., being kicked, beaten, choked, or burned on purpose, having a weapon used against them, etc.) from an intimate partner in their lifetime. Additionally, 16% of women and 7% of men have experienced contact sexual violence (this includes rape, being made to penetrate someone else, sexual coercion, and/or unwanted sexual contact) from an intimate partner. Ten percent of women and 2% of men in the U.S. report having been stalked by an intimate partner, and nearly half of all women (47%) and men (47%) have experienced psychological aggression, such as humiliating or controlling behaviors (pages 7-8).”
Numerous studies identify how the risks for intimate partner violence actually begin in the early years of life (late childhood and teen years). Many programs have been found to be very effective in reducing risks to those receiving various forms of educational and treatment interventions.
The guidelines in this PDF file focus on frequency of physical, sexual, and emotional abuse, which includes a body map to document physical damage. Questions include: have you ever been (or recently): hit, slapped, kicked, or otherwise physically hurt by someone close to you (partner, spouse, close friend), or has anyone forced you to have sexual activities?
Other assessments ask these questions: are you in danger now, is the perpetrator here with you now, do you have a safe place to go to after the treatment, do you feel in danger, are any children in danger, are drugs and/or weapons involved, and how serious have the threats been?
The U.S. Bureau of Justice Statistics reports crime for each year. In 2013 a report was released on Non-fatal Violence, 2003-2012 (retrieved 20 June 2014 SOURCE ). The report shows that about 21 percent of all crime victims were attacked in what has been defined as domestic violence or violence perpetrated by intimate partners, immediate family, or other relatives. Another 32 percent were attacked by a well-known acquaintance and only 38 percent were attacked by a total stranger. The report summarizes US domestic violence trends from 2003-2012:
"Domestic violence accounted for 21% of all violent crime. Intimate partner violence (15%) accounted for a greater percentage of all violent victimizations than violence committed by immediate family members (4%) or other relatives (2%). Current or former boyfriends or girlfriends committed most domestic violence. The majority of domestic violence was committed against females (76%) compared to males (24%). „ A similar percentage of violence by intimate partners and immediate family members was reported to police (56% each). An estimated 49% of violence by other relatives was reported to police. Most domestic violence (77%) occurred at or near the victim’s home. Intimate partner violence resulted in injuries more often than violence perpetrated by immediate family members and other relatives. A weapon was involved in a larger percentage of violence committed by other relatives (26%) than intimate partners (19%) and immediate family members (19%) page 1.
Figure 5 shows the domestic violence trends with the number of attacks per 1,000 people aged 12 and over between 1993-2012. The Intimate partner version of this type of violence has been dramatically reduced in part because of laws regulating police intervention. The re[port reads, "Current or former boyfriends or girlfriends (7.8%) committed a greater percentage of all violent victimizations than spouses (4.7%) and ex-spouses (2.0%). Violence committed by immediate family members accounted for 4.3% of all violent victimizations, and other relatives accounted for 2.4%. The percentage of total violence perpetrated by other relatives (2.4%) was greater than the percentage by the victim’s parents (1.2%), children (1.5%), or siblings (1.6%). These relationships were similar for serious violence and simple assault (page 3)." Figure 5 shows the degrees and processes associated with family violence.
Figure 5. Rate of Domestic Violence in the US 1993-2012*
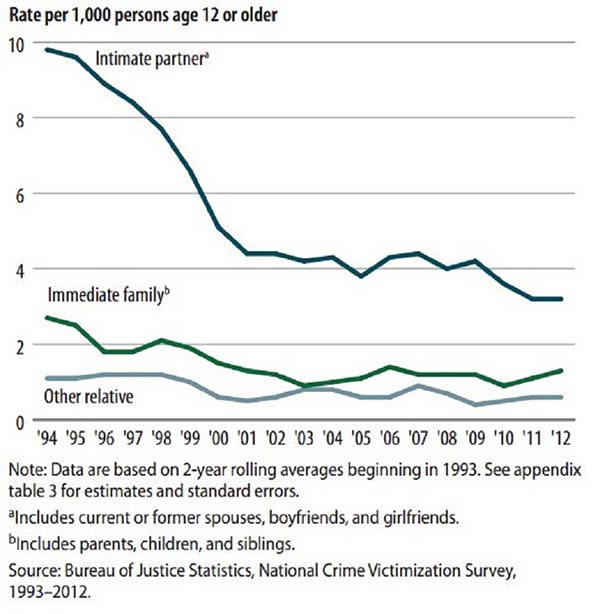
Figure 6. Family Maltreatment Considering Degree of Violence and Conflict.
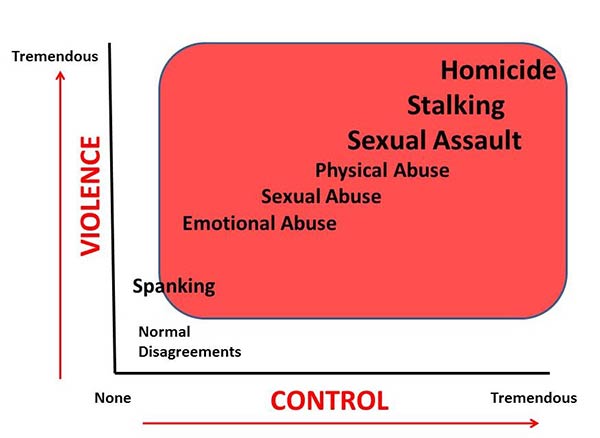
In families, normal disagreements occur. These are typically not at the degree of violence or control that authorities would become involved. Many parents spank their children. This is a two-edged sword. A spanking can be a simple swat. Used rarely and with low levels of violence and control, this would not concern authorities. The other edge of the sword is that some parents use spanking at high levels of violence and control. In the name of spanking they may emotionally, physically, and sexually (really rare) abuse their kids.

I have a friend who went to a family reunion and was slapped 5 times by an angry sister during the reunion. She was 54 during this event. (Let me just say something: when I reference my friends, these are true stories. I try to disguise some of the details, but they are real people. To date I have taught more than 22,000 students in university or college. These stories are real.) All abuse is emotional or has emotional underpinnings because in families we are emotionally connected to each other and because we all filter experience through our emotions.
I am biased about sexual abuse. Fondling, touching, and sexual intercourse are all violence to me, especially when an adult is perpetrating a child. Even verbal sexual comments are inappropriate. To me, children are to be protected and nurtured, not exploited. The laws of all 50 states concur with this opinion. But much goes undetected by authorities. There are homes where boys and girls, teens, and even young adults are violated sexually at some level.
In one extreme case in our state, a girl was beaten so severely that she died. Her parents even beat her in her pelvic area and threw her through a sheetrock wall. Hundreds of similar stories were available, yet hers is in the hands of the criminal justice system and out of the public eye (as are so many cases like it). Except that both parents are in prison, to the public, it is forgotten. Physical abuse includes punches, shoves, bullying, etc. It is extremely common and can lead to murder.
The sexual assault, stalking, and homicide categories of maltreatment are typically considered to be between adults and other adults, but parents do injure children to the point of death. Current spouses, ex-spouses (partners or lovers), and relatives sexually assault, stalk, and/or kill other family members. The first suspect in the murder case of a woman is by default her intimate partner. Once he is ruled out, the police focus on other theories of the crime.
Family violence is common and mostly perpetrated by males on others, but males are also victims of family violence. Even though violent crime has been declining since 1994, males are far more likely to be victimized than females (except in sexual violence). In less common circumstances, women perpetrate violence on men (see M. Carney, F. Buttel, and D. Dutton, 2007, "Women who perpetrate intimate partner violence: A review of the literature with recommendations for treatment," Aggression and Violent Behavior 12 (1): 108-15). There are networks of shelters for men abused by women and/or other men. The easiest way for a man to get help is to call 911. There are online resources that can provide information (Google "shelters" or go to http://dahmw.org for more information).
Spousal and/or intimate partner abuse is extremely concerning to those who try to intervene in family violence. One study using a sample of 16,000 adults in the U.S. reported that 25 percent of women and 7.5 percent of men had been assaulted by their spouse, cohabiting partner, or date. This data yields estimates of over 2 million intimate partner assaults per year in the U.S. (retrieved 23 April 2010 from Patricia Tjaden & Nancy Thoennes, U.S. Dep't of Just., NCJ 181867, Extent, Nature, and Consequences of Intimate Partner Violence, at iii (2000), available at http://www.ojp.usdoj.gov/nij/pubs-sum/181867.htm). Scientists at the CDC estimate that there were over $8 billion in medical costs for spousal violence in 1995 and 8 million lost work days (retrieved 23 April 2010 from Intimate Partner Violence: Consequences SOURCE ).Intimate partner violence used to be called domestic violence. It can be physical, emotional, sexual, threats of violence, or stalking. Stalking is when someone harasses or threatens another repeatedly, even knowing their pursuit is unwanted. Various studies indicate that intimate partner violence is more common among the poor, the unemployed, younger parents, and substance-abusing partners in society (retrieved 4 June, 2014 SOURCE ). The best strategies for intervening include arrest of the perpetrator, protection orders from courts, prosecution of perpetrators, and batterer intervention programs (retrieved 23 April 2010 from http://www.ojp.usdoj.gov/nij/topics/crime/intimate-partner-violence/intervention.htm). Unfortunately, the victim often refuses to follow through on pressing charges.
It is very important to understand how violence and abuse transpire in intimate relationships. A 2006 study identified the nature of control and violence between the two people involved. The researcher, Michael P. Johnson, reported that four categories emerged:
Intimate terrorism is where the individual is violent and controlling, the partner is not. In violent resistance, the individual is violent but not controlling, the partner is the violent and controlling one. In situational couple violence, although the individual is violent, neither the individual nor the partner is violent and controlling. In mutual violent control, the individual and the partner are violent and controlling. (retrieved 26 April 2010 from SOURCE ; Violence Against Women, Vol. 12, No. 11, 1003-1018 (2006): Conflict and Control)
In the 1970s, new models emerged that helped professionals understand and intervene in abuse. These models focused on the cyclical nature of abuse (see Lenore E. Walker, 1979, The Battered Woman, New York: Harper and Row). That means abusers typically cycle in and out of violence with their intimate partners. For example, after the relationship becomes established abusers go through a stage of tension and frustration buildup. These times are filled with perceived offenses by the perpetrator, who begins to define himself as being victimized. Eventually the perpetrator attacks and releases this pent-up anger and hostility. Shortly thereafter he feels remorse and reconciles himself to his family member (victim).
Sometimes there is a phase of calm that lasts until the perpetrator recycles back into the tension and frustration buildup stage again, repeating the violent cycle over and over (see Linda G. Mills, Violent Partners: A Breakthrough Plan for Ending the Cycle of Abuse, 2008, for more details on how to break the cycle as a victim). Why women and some men stay with their abuser is difficult to explain, but it is a major component of successful efforts to intervene. Some have learned that this is part of an intimate relationship -- to suffer and forgive. Others stay because they see no economic possibilities if they did leave. Others stay to minimize the relationship breakup and the impact the harm of that breakup may cause to their children. Communities have responded to this ongoing problem in multiple ways and at multiple levels. Coordinated efforts have been designed to get police, medical personnel, courts, family, and other social agencies working in the same direction for the best outcomes (reduced abuse). The most common model used today to intervene in domestic violence is called the Duluth Model.
The Duluth Model came in the 1980s from Duluth, Minnesota, where an experiment was attempted that united 11 community agencies to reduce violence against women (see http://www.theduluthmodel.org/about/index.html ). This model claims that it is the community that controls abusers (not the spouse), that there are differing types of abuse and each must be responded to in appropriate ways, that socio-economic and historical factors of persons involved must be considered, and that intervention must include perpetrators and victims (retrieved 20June 2014 from The Duluth Model home at SOURCE ).
Critics of the Duluth Model point out the absence of counseling and therapeutic efforts. Other critics argue that it is the court and legal avenues that ultimately protect the victims. Intervention models often include Duluth and cognitive behavioral therapy plus community intervention strategies. One study found that when considering the most common intervention models, there was really no strong indication that one might be better than the other (retrieved 23 April 2010 SOURCE). The Duluth Model and its many variations, when combined with other strategies, are the best way to manage and intervene in family violence cases. One emerging effort designed to encourage abused people to leave the relationship is called the Hope Card Project . This will help people across municipal jurisdictions to transition away from abusers and into abuse-free circumstances.
There is also a concern about the large numbers of elderly abused by younger family members. Family Elder Abuse is the maltreatment of older family members in emotional, sexual, physical, financial, neglect, and other ways, especially where trust was expected and violated SOURCE. Cooper et al. (2008) estimated that 1 in 4 elderly persons may be at risk for abuse in Western nations (see C. Cooper, A. Selwood, and G. Livingston, March 2008, "The prevalence of elder abuse and neglect: a systematic review," Age Ageing 37 (2): 151-60, SOURCE).
Bankrate.com ran an article about the 8 most common financial scams of the US elderly which cost an estimated $billions annually. The National Center on Elder Abuse reports that Care facilities also work diligently to prevent sexual, emotional, physical, and other forms of abuse by employees and family members. This Center estimates about 2 million elderly who've been abused, even though it admits that there is no uniform system in place to track the abuses (retrieved 8 August 2020 from SOURCE.).
Marital Stressors
There are other family tragedies that families must deal with over the life course of the family. The life course of the family can be defined in relation to their time together, children, ages, and work experiences. Young Families tend to be in their 20-30s, they have young children, they are establishing their careers and buying assets, and they have less than a decade together. These families have many stressors that accompany the process of establishing their family. Normative Stressors are expected life events and processes that bring stress by virtue of their nature. Normative stressors get heavy for young families. Having a baby, getting a new job, and buying a home are all normative stressors.
Many married couples experience a noticeable decline in marital satisfaction at the birth of their first child. Judith Wallerstein is quoted as having said, "Each couple must embrace the daunting roles of parents and absorb the impact of her majesty the baby's dramatic entrance while protecting the couples' own privacy" (see The Good Marriage, 1995, NY: Houghton Mifflin). Many researchers have established a decline in marital satisfaction after the birth of a child, especially the first child. The better the couple are as friends, the less the impact the first child has on their marriage. To transition to the role of parents, it was found that couples who work closely and in a mutually supportive manner make the best adjustments (retrieved 20 June 2014 from Marital Satisfaction Across the transition to parenthood Lawrence, E. et al. (2008) J Fam Psychol. Author manuscript; available in PMC Feb 1, 2009. Published in final edited form as: J Fam Psychol. Feb 2008; 22(1): 41–50.doi: 10.1037/0893-3200.22.1.41).
When we bought our first home, we purchased it through friends who were eager to sell and move. They lowered the price for us. Because we got along so well, things went easier for all of us. But it was by far the most stressful experience of our married lives. We spent two weeks arranging our finances, getting all the legal paper work in order, helping them by keeping appointments with inspectors and closing agents, and beginning to pack our belongings. We simultaneously put our mobile home on the market. The day of the closing, minute details threatened the paperwork so much so that we truly reached the point of believing it wasn't going to happen. We eventually signed and succeeded in buying the house. The next day, our home sold and the process of appointments and inspections began from the seller's point of view -- then came the move. Our friends moved out. We helped them clean. Then we moved in. We got all of our belongings into the house by about 11:30 at night. The first night in our house we slept on the floor, exhausted to the core of our souls. Buying this house was a huge boon to us. But even though it was a normal thing for a U.S. family to do, it was very stressful.
Middle Families tend to be in their 30-50s, their children are teens or young adults, they are in mid-career, and they are financially established with a home and cars. Middle families launch children into college, the military, and jobs while maintaining steady earnings. They typically have retirement investments and are paying off mortgages and other loans. As they age into their 50s, they find that some of their married children return home for a short season because of marital or financial hardships. Parents begin to witness the death of their own parents and siblings and are made much more aware of their pending move into the ranks of the elderly. These families have fewer normative stressors than the younger families.
Elderly Families have more freedoms from child-rearing than the younger families have. They are 60-plus and are often grandparents, have their homes paid off, and are looking forward to retirement. Their grandchildren graduate college and become parents in their own right. They have experienced the passing of their grandparents, parents, aunts and uncles, and siblings. They also have begun to face the sober realities of their biological health declines. These families have far fewer normative stressors than younger families.
Acute Stressors are typically unexpected and sudden, and they demand tremendous resources to cope with them. Bankruptcies, illnesses, crime victimization, loss, and natural hazards are just a few of the acute stressors that could impact a family. Wallerstein and Blakesly (1995) also reported that happily married couples had "confronted and mastered the inevitable crises of life, maintaining the strength of the bond in the face of adversity." Stuff happens, and some of it is truly acute and stressful.
In the 1970s, two psychiatrists named Thomas Holmes and Richard Rahe developed a scale that measured life stressors that could have impacted an individual or his or her family over the last three years (see T.H. Holmes and R.H. Rahe, 1967, "The social readjustments rating scales," Journal of Psychosomatic Research, 11:213-218; also see another approach from G.W. Brown and T.O. Harris, 1978, Social origins of depression: A study of psychiatric disorder in women. London: Tavistock). For families in the young family stage, getting married, having a baby, buying a home, or having a parent die ranked as the most stressful events. For middle and older families, having your spouse die, divorce or separating, moving, and being married were among the most stressful events. In this paradigm one of these events can be coped with fairly well if the family members can gather enough resources to meet the challenge. Two or more acute stressors can pile up into your normative stressors and overwhelm you to the point of illness. This happened to me recently. My father died of cancer, we nearly lost an investment that would have financially ruined us, our married son and his wife moved back home with us then had a baby (they both lost their jobs), I had a car wreck, and I was promoted to Assistant Department Chair. This is on top of all the normal life events we have as parents of three teenagers and employees. As Homes and Rahe predicted, I had surgery.
My life is not that bad compared to our friends' lives. Our best friends from junior college suffered an accident in 1991 when one of their 18-month-old twins ran underneath a truck and was instantly killed. This tragic loss impacted them, us, friends, and family. To this day, this has proven to be the most intense stressor they have faced. They survived the loss, but if you were to ask them, it still exists as a tender part of their feelings. How families respond to stresses make a huge difference in their quality of life. Researchers have established that stress can strengthen you or destroy you, depending on how you cope with stressors as individuals or families.
When a series of normal and less significant stressors accumulates, it can have the same effect as a major acute stressor. If both happen together, stress can pile up. Stressor Pile-up occurs when stressful events accumulate in such a manner that resolution has not happened with existing stressors before new stressors are added. Stressor pile-up can be detrimental if adequate resources are not obtained to meet the demands of the stressors (Google "McCubbin's ABCX Models").
My very first pandemic, ever!
During the traumatic pile-up caused by COVID 19 we were trying to complete all our courses online. The pandemic and risks of dying or getting sick were burdensome, the stress of not knowing until 10 days prior, that none of the students and faculty would attend the rest of the semester in-person, and the stress of the wide-spread panic and massive fear-mongering provided nonstop by news agencies; led to many of us becoming very stressed. I was interviewed for an online article which ended up being published by one of our academic advisors for all our students, faculty and staff (see Amanda Hyer 7 April, 2020 at https://www.uvu.edu/news/2020/04/04072020_isolation_mental_health.html ). I ended up sharing an approach to handling stress that I have discovered many years ago when my students and I volunteered to help Firefighters, EMS personnel, Prison Guards and others avoid burn out. It’s called Post-traumatic Growth.
Post-Traumatic Growth (PTG) is a perspective of positive change one takes during crisis. It defines a crisis and the stresses that stem from it as opportunities (albeit unwanted ones). The goal is to anticipate that living on this earth in uncertain and sometimes traumatic life conditions will bring trauma, so plan for it and more importantly plan to grow from it. Unlike the psychological concept of post-traumatic stress disorder, PTG focusses on growth as a way to shift from the passive role into an active, self-directed role. Look for benefits the experience has brought you, plan to avoid it ever happening again, and grow in preparation for any other traumatic experiences you may encounter. I’m not happy I went through a pandemic this year. But I saw my PTSD symptoms piling up and went immediately into growth mode and benefit seeking mode. I also learned every way possible to avoid contracting COVID 19 and plan to be even better prepared in the event of another pandemic before 2035.
This generation of families does not share the same conservative financial tendencies as did the generation of our grandparents. In the U.S., many desire to have what they desire now, even if debt has to be incurred to get it. Now-time Gratification (also called present time) is the individual perspective that seeks immediate satisfaction of their needs, wants, and desires. Delayed Gratification is the individual perspective that has patience and the ability to invest time and efforts now in hopes of a payoff down the road. Delayed gratification is very common among college students, who are willing to put in 4-6 years for the promise of a lifelong career of better earnings and life experiences.
Bankruptcy often occurs among those who are now-time oriented and fail to wisely manage their resources. A Bankruptcy is a federally authorized procedure that allows families (businesses too) to be relieved from liability from their debts and to arrange partial repayments through court-ordered relief strategies. The American Bankruptcy Institute keeps track of bankruptcies in the U.S. and reports hundreds of thousands of bankruptcies each year (SOURCE and see also SOURCE ). The majority of those are non-business consumer bankruptcies. Chapter 7 (quickest and easiest for business and individuals) and Chapter 13 (has a built-in repayment plan) are the two most common forms in the U.S. Bankruptcy does not allow persons to walk away without repercussion.
The 2005 Bankruptcy Abuse Prevention and Consumer Protection Act mandates partial repayments and an 8-year waiting period before refilling (see "Hearing before the Senate Judiciary Committee on Bankruptcy Reform," 109th Cong., 10 February 2005, retrieved 27 April 2010). Consumer misspending and mismanagement of funds contribute to a great deal of bankruptcies, but medical bills are often reported as being the cause for half of all bankruptcies in the U.S. (see SOURCE and for a debate see SOURCE ).
Pregnancy and Delivery
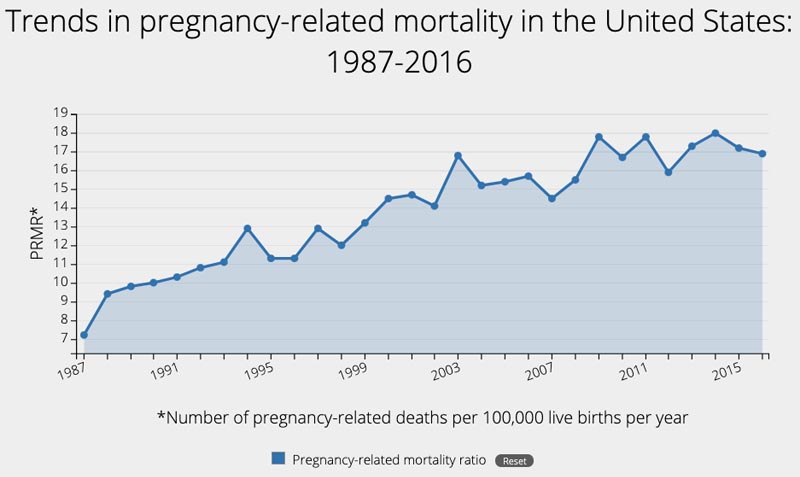
A normal pregnancy takes 9 months or 38 weeks after conception. Most babies are born without complications, but it would be considered extremely risky to try childbirth without professional help. Not every mother, fetus, or newborn child can survive pregnancy and birth. Medical scientists and other research have extensively studied how to keep all individuals involved alive if at all possible. The CDC began tracking maternal mortality decades ago and has recently created a chart identifying pregnancy-related deaths between 1987 and 2016. Figure 7 shows these trends. The CDC noted that a pregnancy-related mortality ratio is equaled the number of deaths per 100,000 live births. In 1987 this was only 7.2/100,000 and in 2016 it had risen to 16.9/100,000 liver births. They describe the reasons for the increase as still being unclear and provided data to so that there are considerable risks.
Figure 7. CDC Trend Line of Pregnancy-related Mortality 1987-2016*
After the 37th week, childbirth can happen at any time. There are three distinct stages of childbirth. In the first stage, the cervix in the lowest portion of the uterus (see chapter 7) begins to dilate and efface. Dilation is the opening of the cervix, which stretches the membranes in such a way that effacement, or the thinning of the cervix, occurs. For the most part, because of contractions of the uterus and muscles surrounding the cervix, the cervix stretches and opens to an undetectable level before the newborn delivers. In the second stage, the baby is pushed down and out, hopefully in the headfirst position and with its nose facing toward the mother's buttocks. The top back (crown) of the baby's head typically presents first, and this is called crowning when it can be seen in the opening of the birth canal. The shoulders deliver first one then the other by lifting then lowering them in such a way as to get one shoulder past the tailbone and the other past the pubic bone. The baby completely exits the mother's body after the shoulders deliver. Once delivered, the baby takes a first breath.
In the third stage, the placenta delivers. If the baby delivers foot or hand first, buttock first, or in any other presentation different from head down and face down toward buttocks, the odds of complications and death increase. The mother also is at risk of complications and death. Some mothers die due to bleeding complications from childbirth (although this is very rare). The CDC reported that in 2014 that "sadly about 650 women die each year from pregnancy and delivery-related complications" (retrieved 20 June 2014 from Pregnancy-related deaths, SOURCE) Given that there are over 4 million childbirths, this number appears to be relatively low. But, one death would be considered too many to the family and friends of the deceased.
Caesarean Sections (C-sections), or the surgical removal of the fetus from the mother through her abdomen, are common when complications are detected. They are much more intensive in terms of healing for the mother, yet far less risky to mother and baby ( more details on C-sections ).During pregnancy a woman will either deliver the baby alive, deliver a baby that died in the womb (still birth), abort the fetus, or miscarry.
Miscarriage (also called spontaneous abortion) is the involuntary ending of the pregnancy by the mother's body, typically considered a default process when or if something is abnormal about the fetus or pregnancy. A woman cannot will her pregnancy into miscarriage, nor can she stop a miscarriage simply by changing her attitude.
Additional Reading
Search the keywords and names in your Internet browser
Adult Survivors of Child Abuse SOURCE
Rape Abuse Incest National Network SOURCE or SOURCE
United Kingdom Abuse Survivors SOURCE
Help for Adult Victims of Child Abuse SOURCE
Kaiser Family Foundation Health Policy Reform SOURCE
World Health Organization on AIDS SOURCE
United Nations Organization on AIDS SOURCE
The U.S. President's Emergency Plan for AIDS Relief (PEPFAR)
White House Factsheet on US Efforts 2013 SOURCE
Center for Disease Control STD/STIs SOURCE