
Chapter 07 - Sexual Scripts
Just a note to begin this chapter; perhaps more than any other topic, sexuality is controversial. Even though it underlies many advertisement themes, is shown independent of any emotional or physical consequences in many TV and Big screen productions, and is commonly participated in outside of marriage, we are raised not to talk about it much. Many of us are even taught that religions are very strict on how sex is exclusively for married people, yet very few of us had the luxury of having our own parents teach us about it.
For some religious believers, it brings family shame to have sex outside of marriage. For others, the fear of God’s retribution shapes their very thinking about what sex is and how we should participate in it. I am strikingly aware of this and deeply committed to being as objective as I can. Rest assured, my goal is not to get you or anyone you know into a risky situation at any level. I am admittedly conservative and biased, but this chapter is not about me. It is about you!
My goal in teaching you in this chapter is two-fold: first, I want you to understand your own sexuality, body, and experiences; second, I want you to do what most US parents don’t do—I want you to teach your own children about sex and to do so with an understanding of the critical information they need to know so that they can learn about their own sexuality, body, and experiences. It would be arrogant and ill-advised for a professor to tell students their sexual values, so I won’t. It would be ill-advised for a parent to avoid telling his or her children about sexuality. So, please do so if and when you have children in their formative years at home.
A script is what actors read or study and what guides their behavior in a certain role. A script is a blueprint for what we "should do" in our roles. Sexual Scripts are blueprints and guidelines for what we define as our role in sexual expression, sexual orientation, sexual behaviors, sexual desires, and the sexual component of our self-definition. All of us are sexual beings, yet none of us is exactly identical to another in our sexual definitions and script expectations. Having said that, keep in mind that we are not just born with sexual scripts in place. They are learned. Sexual socialization is the process by which we learn how, when, where, with whom, why, and with which motivations we are sexual beings.
We are all born with drives which are biological needs that demand our attention and behavioral responses to them. The most powerful drives are: circulation; breathing; voiding our urine and other waste; eating; drinking; sleeping; and sexual involvement. Sexual drives are biological urges to participate in sexual activity in certain sexual roles.

Sexual scripts, once learned, will shape how that drive is answered. Sexuality is learned via culture and socialization. There are as many unique sexual scripts as there are people, yet some of these scripts have common themes and can be viewed as a collective pattern or trend in the larger social level. Many of us learn our sexual scripts in a passive way. In other words, we don’t learn from experience, but from a synthesis of concepts, images, ideals, and sometimes misconceptions. For example, the commonly held belief that men and women are two different creatures, perhaps from different planets was a very successful fad in recent years that led an entire generation to believe that men might be from "Mars" while women might be from "Venus" (John Grey, various self help books).
Today more and more in the US have less religious values and more diverse experiences with sexuality. So much of the younger generation’s focus on sex is about the orgasm. An Orgasm is the sexual climax that accompanies sexual intercourse and includes muscle tightening in the genital area, electrical sensations radiating from the genitals, and a surge of a variety of pleasure-producing hormones throughout the body. Many cultures have records of sexual expression and some even have records of sexual pleasure maximization (see Karma Sutra).
Some traditional sexual scripts that have been studied and have found to include a number of problematic assumptions including: the man must be in charge; the woman must not enjoy (or let on that she enjoys) the sexual experience; the man is a performer whose skills are proven effective upon arrival of his partner’s orgasm; men are sexual while women are not; women can’t talk about it and turn to men for sexual interests and direction, and finally sex always leads to intercourse and a female orgasm (her orgasm being proof of his sexual capacity). Numerous studies have shown that most of these traditional scripts are not: realistic, healthy, conducive to open communication, nor negotiation of sexual needs and desires for couples. In sum, these traditional notions can be an undermining influence in a couple’s intimacy. More contemporary scripts include these simple ideas that:
- both partners need to learn to take ownership of the couple’s sexual experiences
- both partners need to learn to communicate openly and honestly about their feelings
- both partners need to learn to meet one another’s: desires, needs, and wishes while making sure that their own needs are being met
Many people think of male versus female reproductive and sexual body parts in terms of opposites. In sexual matters, men and women are very much alike from a physiological and biological point of view. We are even alike in our fetal development with our genitals developing from identical tissues, regardless of being male or female. Have you ever wondered why a pregnant woman can’t get an accurate ultrasound until the second month to determine the fetus’s sex being male or female? In part, technicians want to give the fetus enough time to develop genitals that coincide with the particular sex of the baby. More importantly, the fetus has identical genitals until about the 5-6th week. That means it would require a DNA test to distinguish which sex the fetus is up until that point.
Sexually, males and females start with identical genital buds that eventually form the male or female reproductive organs. Figure 1 briefly discusses the development of male and female sexual parts from very similar genital pelvic tissues. Please note that sexual development is a natural yet extremely complex process that yields a mostly predictable outcome among newborns. That means most females are born with nearly identical sexual parts. Likewise most males are born with nearly identical parts.
Figure 1. Similar Sexual Development in the Male and Female Fetus

Figures 2a and 2b show an artist’s depiction of the tissues that biologists would use to identify the developing genitals of males and females. I have to express thanks to my Senior Research Student, Sam Jones who volunteered to draw these for this free online book.
Figure 2a. How Male and Female Reproductive Parts Generate from the Identical Fetal Tissues-Undifferentiated

Figure 2b. How Male and Female Reproductive Parts Generate from the Identical Fetal Tissues-Differentiated

With an XY male genetic configuration, the glans area will develop into the penis. The urethral fold will form the urethral meatus or opening in the penis. The urethral groove and lateral buttress will fold onto itself and fuse into the shaft of the penis with the urethra connecting the bladder to the urethral meatus or opening of the penis. The anal tubercle will form into the anus and external sphincter. The male glands: prostate, Cowper’s, and seminal vesicles develop in another process as do the testicles which develop inside the abdomen then drop into the scrotum.
For the XX female genetic configuration, the glans becomes the clitoral glans; the urethral fold becomes the urethral meatus; the urethral groove and lateral buttress become the labia minora and majora (labia means lips); and the anal tubercle becomes the anus and external sphincter. The vagina, cervix, ovaries, and uterus form from other tissues. Interestingly, ovaries develop inside the abdomen. These basic fetal tissues differentiate because of the X or Y. In adult sexual partners these sexual parts function in very similar ways even though their placement and structure differ.
Everyone matters and everyone should be included. This is a bold assertion that everyone should be included. There have been decades of focused efforts to create a cultural shift away from excluding certain categories of people and toward the inclusion of all the diverse categories of the human experience that can be found in modern society. The Gay & Lesbian Alliance Against Defamation (GLADD) identifies in detail some of the gender-related definitions and concepts that can be very helpful for those wanting to better understand the many diversities of the human experience while treating individuals with dignity and respect (SOURCE)
As is mentioned in Figure 2, not all fetal sexual development occurs uniformly. Though not discussed here in great detail there are 5 common sexual development variations reported among newborns: Turner ’s syndrome, Klinefelter’s Syndrome; Androgen Insensitivity Syndrome; Fetally Androgenized Females; and DHT-deficient Males. Simply search the Internet for these images and explanations. In most cases of fetal development, sexual development is predictable and follows the above mentioned pattern of originating from nearly identical tissues.
Sexuality is important to us because it represents an activity that is a rite of passage into adulthood, because it is very pleasurable, and because it reinforces our roles and aspirations as males and females. Yet, sexuality is truly a passive part of our daily lives. What does that mean, "passive part of our daily lives?" Samuel and Cynthia Janus published The Janus Report on Sexual Behavior in 1993 (Wiley and Sons ISBN 0-471-52540-5). They studied a scientific sample of 2,765 men and women and reported some general trends in US sexual practices and patterns. They found that age-based estimates indicate a great deal of similarity in sexual frequency between age groups with 2-3 sexual encounters per week.
Sex is a minor (yet important) part of our daily time allocation. People with a sexual partner available have sex about 3 times per week; taking about 25 minutes per experience (I am fully aware that some people have more sex than others and that circumstances impact more or less frequency and or duration. Yet, we can make estimates that illustrate the point). That means about 75 minutes per week or 3,900 minutes per year. Divide 3,900/ 60 minutes and it equals about 65 hours per year having sex. At first glance that sounds like a great deal of time allocation.
But, keep in mind that in comparison, most of us spend most of our lives doing nonsexual things. Consider these estimates: if the average person sleeps about 8 hours in a 24 hour period; works 8.5 hours; eats 1.5 hours, commutes .5 hours; watches TV for 3 hours; and about 3.5 for miscellaneous activities, then compared to routine non-sexual activities, sexual intercourse comprises a relatively small portion of our time. Table 1 shows some estimated daily and yearly hours spent in various activities. Sexual intercourse doesn’t happen 4 days out of the 7-day week and only happens for a brief interaction during the other 3 days of the week.
Table 1. Daily and Yearly Hours Spent in Various Activities for An Average Person
| Activities | Daily Hours=24 | Yearly Hours=8,760 |
|---|---|---|
| Sleep | 8.0 | 2,920.0 |
| Work | 8.5 | 3,102.5 |
| Electronic Media | 6.0 | 2,190.0 |
| Eating | 1.5 | 547.5 |
| Commuting | 0.5 | 182.5 |
| Miscellaneous | 2.32 | 846.8 |
| Sexual Intercourse | 0.18 hours (About 11 minutes per day average) | 65.0 |
Relatively speaking sexual intercourse is a passive part of the average person’s life accounting for only 65 yearly hours of involvement per year. Many people refrain from regular sexual intercourse until their twenties and are less likely to participate in it if they are not married than are married people. These estimations don’t take into account those with no sexual partner and those who abstain from sexual intercourse. The average would be much lower if those categories of people were averaged into the equation.
To understand our own bodies and also understand enough about sexuality to teach our children, we must understand the basics of female and male anatomy. Figure 3 shows an artist’s depiction of a cross section of female reproductive and sexual anatomy. The clitoris is extremely sensitive and is protected by the clitoral hood (not shown here). It sits above the vagina. In females, urine exits the body at the external urethral orifice (also called meatus). The vaginal orifice simply means the opening to the vagina itself. The labia are in two places, closer to the vaginal orifice (labia minora) and further away from the vaginal orifice (labia majora).
The urinary bladder sits behind the pubic bone and during urination travels an inch or two out of the body via the external urethral orifice. In the back and top of the vagina sits the cervix. The cervix is simply the window into the uterus. It is round, muscular and thick and has a small opening in it. The cervix is the bottom portion of the uterus (the uterus is where a fetus or baby would grow and develop during pregnancy).
Figure 3. Female Reproductive and Sexual Anatomy, Cross-sectional View

The uterus leans forward toward the pubic bone. Inside the uterus on the left and the right sides are 2 small openings where the fallopian tube connects the ovaries to the uterus. There are two ovaries that have thousands of eggs in them at birth. A woman may release as many as 450 eggs during her reproductive years. After an egg is released from the ovary (ovulation), the fallopian tube carries the egg from the ovary down to the uterus. When pregnancy occurs it is often because sperm met the egg in the fallopian tube and fertilized it. Later, if the fertilized egg travels down the fallopian tube and implants into the uterus, then conception has taken place.
The vagina is approximately 3 inches long and is made of tissues that are epithelial and mucosal. This means that when blood flow increases to the pelvis the vagina produces a lubricant in the form of moisture. The vagina is not hollow in the sense that a tube is round and hollow. The vagina is relatively flat and has potential space not constantly open space. The vagina has a band of pelvic floor muscles that surround it. One set of muscles is called the puboccocceygeus muscle (PC muscle) which is located approximately 1 inch inside the vagina and which also plays a role in sexual pleasure for both partners.
To truly understand how these parts function during sexual intercourse, we need to consider a research-based paradigm developed by Masters and Johnson years ago which they called the sexual response cycle (see Master, W. & Johnson, V. 1966, Human Sexual Response; Boston: Little Brown). The Sexual Response Cycle is a model that explains how most people experience three phases when they engage in sexual intercourse: excitement, plateau, and then orgasm.
Masters and Johnson are quick to point out that each individual has a unique and varied sexual response so much so that no two sexual encounters would be expected to be perfectly identical between the same people. Nevertheless, these three phases are very common among most people. You may want to search the Internet for Kaplan’s model and Master’s and Johnson’s four-phase model.
As sexual intercourse begins here is what happens to both males and females as they pass through these three phases: Excitement Phase is when blood flow to pelvis bringing more lymphatic fluid and plasma to the region. Because of hormonal and psychological stimuli there is generally swelling in the sexual parts. While this is happening, the Plateau Stage begins which is when more hormones are released, moisture increases, heart rate increases, intensity of sensory perception increases (touch, smell, sight, hearing, and taste). In the Orgasm Phase an electrical build up of energy is released that is associated with a rhythmic contraction of: the pelvic floor muscles, the urinary and anal sphincters, and of various glands for males. This is called an orgasm. After the orgasm finishes, resolution eventually allows the sexual parts to return to pre-excitement conditions. These are almost identical in every way between males and females, except that there are differing sexual parts for each.
Thus, a sexual response in a typical female would typically follow a pattern similar to this one. In the excitement phase, blood and lymphatic fluids increase swelling inside the vagina. Hormones are secreted which lead to a mild uterine contractions which raise the uterus away from the pubic bone. The labia swell and the clitoris becomes hard. The vaginal tissues secrete moisture and the vagina itself lengthens and expands slightly inward.
The plateau phase begins as excitement continues. This causes the labia to become fully swollen, the clitoris to recede under the clitoral hood, and the uterus to become fully elevated (the hormone is called Oxytocin). The vagina is fully lengthened into the body and just before orgasm lubrication ceases. During orgasm, the pelvis of the female experiences a series of contractions which occur every 8/10ths of second and can number anywhere from 1-20 or more in the sequence. The contractions include: anal and urinary sphincter contractions; the smooth muscles in the inward portion of the vagina contraction, the puboccocceygeus muscle contraction, the uterine contractions which cause the uterus and cervix to dip down into the vagina, and general muscles contractions in the body.
Also, an electrical sensation surges from the clitoris radiating throughout the body and stimulates the pleasure centers of the brain and a release of the hormone called Oxytocin. When the orgasm ends the body eventually returns to its pre-excitement state. In general, females have more capacity to experience more contractions over a longer period of time than do males. Females have been found to have much more capacity for sexual intercourse than males. This means females can have more sexual intercourse, more often, and with more orgasms than can the average male.
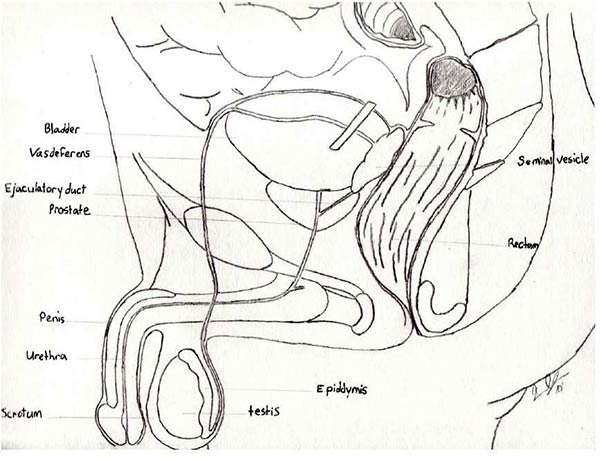
The male anatomy is presented in Figure 4 below. The male has a penis which is comprised of 3 spongy-like tissue columns that engorges with blood during excitement. A cross-section of the penis shows two outer columns and one column on the underneath side. The average male penis is just that—average. About 4-6 inches reported by Masters and Johnson (Same reference as above). Some are smaller. Some are larger. Since the vagina is 3 inches in length and has very sensitive regions near the outside of the vagina and not so sensitive regions deeper inside, the average male can satisfy the average female in heterosexual intercourse. Urine passes from the urinary bladder and exits at the external urethral orifice at the tip of the penis. The penis is attached inside the body to the pubic bone.
There are two testicles inside a pouch called the scrotum. One testicle sits higher than the other. On the back of the testicle is a storage compartment where mature sperm end up before ejaculation. This is called the epididymis. There is a muscle called the dartos muscle (not shown) which elevates and lowers the testicle based on temperature and sexual pleasure. Sperm grow best at about 91 degrees Fahrenheit and most males are at about 98 degrees, so the dartos will raise and lower the testicles if in colder or warmer temperatures.
The testicles produce about 125-250,000,000 sperm every 3-4 days. More importantly, the testicles produce the sex-drive hormone called Testosterone. In males and females, higher levels of testosterone typically mean a higher sex drive (another similarity). The vas deferens will eventually carry the sperm from the epididymis out of the body during the orgasm. The prostate gland swells during excitement and fills with prostatic fluid. The seminal vesicle located above the prostate gland also swells and produces a fluid filled with natural sugars.
For males, in the excitement phase, blood and lymphatic fluids increase swelling inside the prostate, seminal vesicle, testicle, scrotum, and the penis. Hormones are secreted which lead to a higher volume of blood flowing into the spongy tissue columns of the penis than flow out. The penis erects this way (sometimes the penis will leak fluid and/or sperm before the orgasm). The scrotum and dartos muscle draw both testicles up toward the pubic bone pressing the epididymis upward. As stimulation continues the swelling and fluid production continues to increase.
Figure 4. Male Reproductive and Sexual Anatomy, Cross-sectional View
The plateau continues until just before the orgasm. When orgasm begins for males the penis is most erect. Males reach a point of no return in their orgasms (females do not). The ejaculation of sperm and fluids will continue in males, regardless of continued or interrupted stimulation. Females would experience an interruption of the orgasm when stimulation is interrupted. For males, the orgasm also includes a series of contractions which occur every 8/10ths of second and can number anywhere from 1-10. Most males will have 5-6.
The contraction includes: anal and urinary sphincter contractions; prostate and seminal vesicle contractions, dartos and scrotum contractions, pelvic floor muscle contractions; penile contractions; and a rhythmic sequence of these in such a way that the ejaculate is expelled from the body out through the penis. The sperm are released from the epididymis and travel through the vas deferens up and around the bladder then through the ejaculatory duct (where it picks up prostate and seminal fluids) and finally out of the penis. An electrical sensation surges from the prostate gland throughout the body and stimulates the pleasure centers of the brain and a release of the hormone called Oxytocin. For males and females Oxytocin brings a feeling of emotional connection.
After an orgasm, males may continue to experience an erection, but will have to wait a while for the central nervous system to reset before they can ejaculate or orgasm again. Most males wait less time when younger and more time when older. For males an ejaculation during orgasm would be expected. But, sometimes ejaculations happen with or without orgasms and orgasms may happen without ejaculations.

Even though the physiological component of sexuality is common between males and females, the male and female sex drives are NOT identical. Studies consistently show that sexual desire for women is more sensitive to the context (meaningful or intimate connection) and the social and cultural environment (quality of relationships, stresses of the day, etc.). Generally speaking most men seek more sex than most women throughout most of the life span. Also, most men are more easily aroused by visual stimulation than are most women.
The Janus Report reported that 65 percent of men have an orgasm every time during love making while females reported a much lower 15 percent every time. About 46 percent of women report "often" having an orgasm during love making compared to only 28 percent of men (Page 86, Table 3.28). These sex drive differences also emerged in self-reported masturbation frequencies. About 55 percent of men and 38 percent of women masturbate on a daily-monthly basis (Page 77, Table 3.21). Another study indicates that solo masturbation is a practice commonly found among married people (see Laumann and Janus).
A more recent 2017 survey of U.S. adults and their sexual frequency indicated that there was an overall reduction in sexual frequencies from 1990 to 2010, likely because there were more singles during that decade and singles have less sexual frequency than married or partnered adults. This study also confirmed the known pattern of sexual frequency declining from about age 50 and later (Twenge JM, Sherman RA, Wells BE. Declines in Sexual Frequency among American Adults, 1989-2014. Arch Sex Behav. 2017;46(8):2389-2401. doi:10.1007/s10508-017-0953-1). Another 2017 study considered sexual frequency of adults comparing Gen X, Gen Y, and the youngest generation they called “iGen.” These researchers reported among those born in the 1990s, 15 percent had not had sexual intercourse since turning 18+ and those born in the 1960s only report 6 percent. (Twenge JM, Sherman RA, Wells BE. Sexual Inactivity During Young Adulthood Is More Common Among U.S. Millennials and iGen: Age, Period, and Cohort Effects on Having No Sexual Partners After Age 18. Arch Sex Behav. 2017;46(2):433-440. doi:10.1007/s10508-016-0798-z ). They concluded that those born more recently had far less sex after age 18+ than those born before 1990.
Numerous studies show that men and women enjoy sex most in a meaningful relationship, typically a long-term committed one. These studies indicate that the pleasure is more meaningful and enjoyable in long-term committed relationships. Figure 5 shows a pleasure and intimacy continuum for both sexes. Those who abstain from all sexual activity are in the lower left corner with no intimacy and no pleasure. Those who solo masturbate (by themselves) derive pleasure without intimacy. Those who purchase prostitution services derive pleasure, yet have very little intimacy. Finally, those who have one-time sexual encounters in a "one-night stand also derive pleasure with little intimacy over time.
Figure 5. Pleasure and Intimacy Continuum for Both Males and Females

For married or cohabiting couples, sexual intercourse includes both pleasure and intimacy. Newlyweds have their honeymoon night and sex becomes a rite of passage that marks the beginning of their full emersion into the marital relationship. In time husbands and wives have sex for many of the other reasons listed in Figure 5. Sometimes one spouse has sex to meet the needs or wants of their partners. At other times sex is a healthy and fun stress relief. Sometimes sex is a convenient way to be affectionate as a giver and a receiver. In relationships, sexual intercourse has many functions including reinforcing commitment and loyalty with one another. To give and receive is pleasurable and bonding during sexual intercourse.
Some couples seeking parenthood will have sex to pleasure themselves while getting pregnant. Many report enhancements of intimacy with less focus on pleasure at moments such as these. Others get distracted because sex becomes goal-oriented rather than simply expressive while trying to make a baby. For long-term relationships that have endured challenges such as: hardship, betrayals, offenses, anger, arguments and ultimately forgiveness; sexual intercourse takes on a profoundness of its own. Those who have short-term relationships miss out on the intimacy payoff that sex provides to those in long-term relationships. Sex becomes a unique way of enhancing trust and closeness while sometimes providing sexual healing to wounded egos and feelings.
Extramarital affairs are intimate relationships with a person other than one’s spouse that may be sexual or nonsexual. Most US extramarital affairs are sexual and non-consented to by one’s spouse. In spite of a variety of estimates on how many married people were ever unfaithful to their spouse, all scientific studies have found that men were more likely than women to have an extramarital affair and that most men and women do NOT ever have an affair.
Marital infidelity has been and continues to be disapproved of by the general public. Many in the US who disapprove of affairs, simultaneously understand the frailties of the human experience and sympathize to some degree with those who make this "mistake." Such was found to be true with politicians, movie and TV stars, and sports celebrities (you can pick any one from the online list available on the Internet when you search "celebrity affairs"). Affairs don’t always lead to marital or relational dissolution. But, in most cases it is better if the offending spouse or partner confesses the infidelity rather than simply gets caught.
Human beings are socialized into their adult roles and learn their sexual identities along with their gender roles, work roles, and family roles. Sexual Orientation is the sexual preference one has for their partner: male, female, both, or neither. There are a few common sexual orientations that can be seen at the societal and personal level. Heterosexuality is the sexual attraction between a male and a female. Homosexuality is a sexual attraction between a male to another male or a female to another female. Bisexuality is a sexual attraction to both male and female sexual partners.
There is a difference in these three dimensions of sexuality: sexual orientation, sexual desire, and sexual behaviors. Sexual desire is the attractions we have for sexual partners and experience that exist independent of our behaviors. Sexual behaviors are our actual sexual actions and interactions. It is important to note that orientations, desires, and behaviors are not always the same thing. They do overlap at times. For example, a heterosexual male may have had a homosexual experience in the past, or not. He may at times desire males and females regardless of his actual sexual activities. A lesbian female may have had a short-term heterosexual relationship, yet define herself as a lesbian.
When considering the congruence of these three concepts it is helpful to use visual aids. Figure 6 below shows how sexual orientation, desires, and behaviors are at times: congruent, meaning they correspond directly with each other; or incongruent, meaning they do NOT correspond together with each other. These three dimensions of our sexuality are surprisingly incongruent among adults in the US society.
Figure 6 Sexual Orientation, Desires, and Behaviors: A Venn Diagram
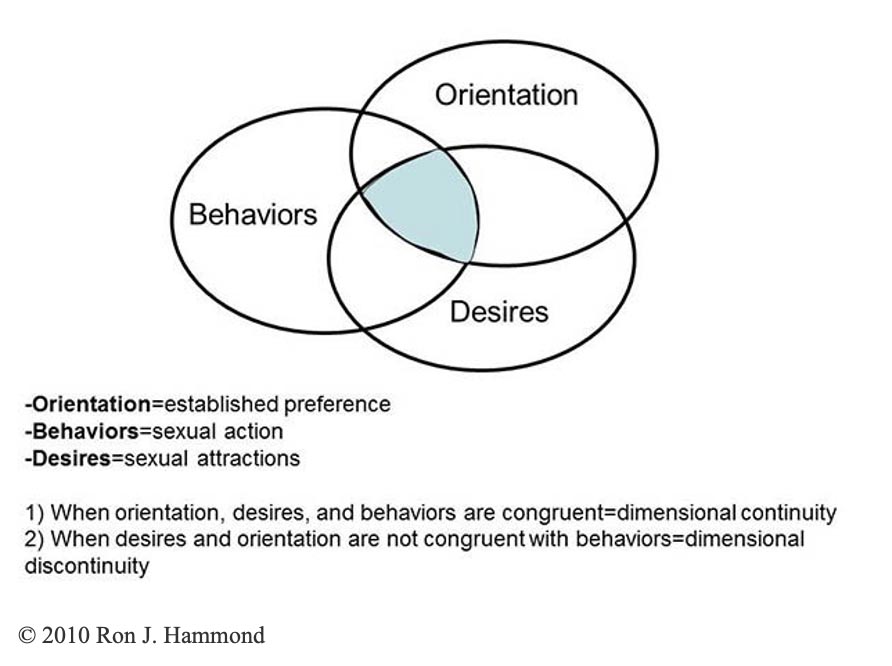
When orientation, desires, and behaviors are congruent that implies dimensional continuity, meaning there is congruency between the three sexual dimensions of: orientation, desire, and behaviors. This is very common and much of the US population has dimensional continuity….. Yet, when desires and orientation are not congruent with behaviors it implies dimensional discontinuity.
The proportion of the US society that is homosexual varies because of the difficulty in defining how to measure it. If researchers ask people their sexual behaviors then the proportion of the population having sex with a same-sex partner is lower than the proportion having ever had sex with a same-sex partner. One researcher, Tom Smith, 2003 reported that:
"However, a series of recent national studies (Table 8A) indicate that only about 2-3% of sexually active men and 1-2% of sexually active women are currently engaging in same gender sex (Page 7)" and that "Studies of male and female homosexuality both in the United States and Europe regularly find a higher proportion of males are gay than the share of females who are lesbian (page 8)." (see American Sexual Behavior: Trends, Socio-Demographic Differences, and Risk Behavior; National Opinion Research Center University of Chicago; GSS Topical Report No. 25; Updated April, 2003)
In another interesting report Joseph Fried studied the General Social Survey (GSS) for specific periods of time and found that using various years of the General Social Surveys found that among US men, 6.6% of Democrats and 2.1% of Republicans had sex with another man in the last 12 months (see Fried, Joseph, *Democrats and Republicans - Rhetoric and Reality* (New York: Algora Publishing, 2008, 10. Figure7 and for even more understanding SOURCE ).
Edward O. Laumann et al wrote the largest sociological study of US sexuality ever published. (1994, The Social Organization of Sexuality U. of Chicago Press ISBN 0-226-46957-3). In this book he wrote about the prevalence of self-identified sexual orientations. Laumann and the other researchers surveyed about 3,400 respondents. By far, most members of US society are heterosexual. Laumann avoided the use of the words, "heterosexual or homosexual." Their data was collected by asking about behaviors or how many male or female partners a respondent had sex with in the past (page 292:note 9). They found that 7.1 percent of males and 3.8 percent of females had ever had sex with a partner of the same sex (page 294).
Laumann also reported that over 96 percent of males and 98 percent of females identified themselves as heterosexual. Only 2 percent of males and 0.9 percent of females identified themselves as homosexual, while 0.8 percent of males and 0.5 percent of females reported bisexuality (page 311 Table 8.3B). The Janus Report also reported their findings on sexual behaviors and sexual orientation. Their sample reported 22 percent of men and 17 percent of women said yes to the question, "Have you had a homosexual experience (page 69 Table 3.14)."
Janus also reported that 91 percent of men and 95 percent of women claimed to be heterosexual; 4 percent of men and 2 percent of women claimed to be homosexual; and 5 percent of men and 3 percent of women claimed to be bisexual (Page 70, Table 3.16). Heterosexuality is by far the most common identification in studies where respondents are asked to identify their sexual orientation.
Yet, heterosexuals may have had a variety of sexual experiences in a variety of context and still consider themselves to be heterosexual in spite of dimensional discontinuity or continuity. Generally speaking Janus and Laumann found that the US is a very sexual nation. They reported that very few men and women reported never having had vaginal sexual intercourse (less than 5 percent). They reported that men typically have sex sooner than women and that most had sex by age 20. Janus specifically reported that only 9 percent of men and 17 percent of women had NO sexual experience before marriage (page 87, Table 3.29).
Sexual orientation, desires, and behaviors have become extremely politicized. The largest sexual political action committee is the Human Rights Campaign which emerged in the 1980s as a "Gay Community" rights organization. LGBT and LGBTQ have replaced Gay Community as the collective acronym. LGBT stands for Lesbian, Gay, Bisexual, and Transgendered and occasionally Queer is added by some interests groups. The Human Rights Campaign has become the central political action organization for LGBTQ interest groups. On this Website, under "Issues" it lists: Aging, Coming Out, Hate Crimes, Health, Immigration, Marriage & Relationship Recognition, Military, Parenting, People of Color, Religion & Faith, Transgender, Workplace, and Youth & Campus Activism.
The "marriage and relationship recognition" became an emotionally charged political issue during the California Proposition 8 referendum and constitutional amendment that Passed November 2008. Because it passed the California Section 7.5 of the Declaration of Rights to the State Constitution now reads, "Only marriage between a man and a woman is valid or recognized in California." This set a strong national precedence against rights to same sex couples to have legally recognized marriage en par with heterosexual married couples. Estimates are that over $80 million was spent on this proposition alone on both the for and against efforts (SOURCE).
The Prop 8 initiative originated from another political action committee called ProtectMarriage.com (http://www.protectmarriage.com/ ). Under the "About Us" link it self-describes as a "…broad-based coalition of California families, community leaders, religious leaders, pro-family organizations and individuals…to restore the definition of marriage as between a man and a woman." Both Proposition 8 and the Defense of Marriage Act (SOURCE) were essentially struck down by the US Supreme Court in 2013. The battle over same-sex marriage rights in the US is far from resolved, but more importantly there is no indication that even the slightest of common ground can be found much less reconciliation obtained for both sides (to read the latest developments SOURCE).
A 2016 study examined how many adults in the United States had experienced at least 1 same-sex, sexual experience in their lifetime. (see Twenge JM, Sherman RA, Wells BE. Changes in American Adults' Reported Same-Sex Sexual Experiences and Attitudes, 1973-2014. Arch Sex Behav. 2016;45(7):1713-1730. doi:10.1007/s10508-016-0769-4 ). As we close this chapter, I want to include a quote from the article’s abstract which concisely summarizes their findings that the clear majority of U.S. adults had not experienced a same-sex, sexual experience in their lifetimes but that a significant percentage had. The abstract reads:
“We examined change over time in the reported prevalence of men having sex with men and women having sex with women and acceptance of those behaviors in the nationally representative General Social Survey of U.S. adults (n's = 28,161-33,728, ages 18-96 years), 1972-2014. The number of U.S. adults who had at least one same-sex partner since age 18 doubled between the early 1990s and early 2010s (from 3.6 to 8.7 % for women and from 4.5 to 8.2 % for men). Bisexual behavior (having sex with both male and female partners) increased from 3.1 to 7.7 %, accounting for much of the rise, with little consistent change in those having sex exclusively with same-sex partners.”
While same-sex “experimenting” or curiosity-based sexual experiences are present in contemporary U.S. Society, they in and of themselves most often do not contribute to a participant eventually coming out as an heterosexual or LGBTQ person later in life. This principle is important to end on—no studies have found any cause for either heterosexuality, homosexuality, lesbianism, Queer, trans-gendered, intersexed or bi-sexual self-identification. I doubt that any scientific research ever will (just my professional opinion).
I also caution those who think that there might be a “cause” to any individual’s personal or sexual identity. Looking for causes implies that once the cause is identified it could be mediated and perhaps stop someone from ever becoming a heterosexual or LGBTQ person. The human socialization experience is not “cause-and-effect” that way. Biologists know that contamination after exposure to the specific virus in the “Corona Virus” category could lead to an infection with a Corona Virus-specific diseases such as COVID 19; SARS-CoV-2, or MERS (See more information at SOURCE).
We don’t have choices to become ill or not once contaminating viruses invade our bodies. We don’t have unique personal histories of trauma, grief, successes, emotions, relationships, and other human-based subjective aspects of the choices we do make. Likewise, we can’t choose our sexuality like we choose our political party. Looking for causes to people’s lifestyle and identity traits is the wrong way to approach other people and it lacks the inter-personal respect we absolutely need to develop and use in our modern complex social lives. In other words we need more who are looking for sincere, compassionate, genuine and non-judgmental friendships; and not looking to judge (this is just my opinion).
Interestingly most in the US would never oppose an individual’s choice or orientation when it comes to sexuality. This and other conservative interest groups like it have formed to advocate for conservative legislation and policies in the US and Abroad. None, on either side of sexual rights, assumes that this oppositional battle for rights, laws, and policies has ended. Many see the stakes as being higher than ever in the current sexual politics scene. We’ve included two personal assessments to help you understand where you learned about sexuality and how better to distinguishes television’s messages about sexuality.
Where I Learned About Sex and Reproduction
Next to each item below, place the letter which corresponds to the appropriate place of origin for your sexual knowledge. Use the following categories: M=Mom, D=Dad, OF=Other family, F=Friends, TV=Television, SC=School/College, R=Religion, B=Books I=ve Read, P=Partner/s, or DK=Don=t know where or did not know about it. You may list multiple origins if they apply. Simply place the one which applies the most first.
____ 1. My sexual/reproductive organs
____ 2. My sexual preferences
____ 3. Conception and how it happens
____ 4. Self-pleasuring, stimulation
____ 5. Pregnancy, nine months gestation, and how it happens
____ 6. Childbirth and how it happens
____ 7. Sexually transmitted diseases
____ 8. Types of contraception
____ 9. The mechanics of sexual expression
____10. What uterus, ovaries, and vagina are and how each function
____11. What penis, testicles, and scrotum are and how each function
____12. Why and how breasts develop for women and how breasts function
____13. What a monthly period is, and how and why it functions
____14. Why sex is Aright@ sometimes and Awrong@ other times
____15. My parent’s sexual values
____16. What a sexual climax is and how it happens
____17. How I feel about love, commitment, and sex
____18. How to prevent pregnancy
____19. How to prevent the spread of diseases
____20. That sex on TV is not always representative of sex in real life experience
____21. The social and cultural pressures for or against sex
____22. Various sexual techniques and practices
____23. What a man is "supposed to do" in bed
____24. What a woman is "supposed to do" in bed
____25. What menopause is, why and how it happens
____26. Why promiscuous people often get a "reputation"
____27. Why, with whom, where, when, and how I choose to have sex
____28. What sex means to the relationship
____29. The role of kissing in sexual expression
____30. The role of touch and caress in sexual expression
____31. My own sexual boundaries (what I want and don=t want)
____32. My personal values on sex
____33. My values on abortion
____34. What virginity means to me
____35. What abstinence means to me
____36. The risks of premarital sex
____37. The occurrence of sexual violence, rape, & abuse
____38. The effects of sexual hormones on males and females
____39. The processes associated with puberty, dreams, & fantasy
____40. The point of view taught in my religion
Once you have completed this assessment, place the item number into the corresponding origin boxes below. If you used more than one origin for an item, place that item in both boxes.
| Category | Statement Number | Total |
|---|---|---|
| M=Mom | # | |
| D=Dad | # | |
| OF=Other Family | # | |
| F=Friends | # | |
| TV=Television | # | |
| SC=School/College | # | |
| R=Religion | # | |
| P=Partner/s | # | |
| B=Books I've Read | # | |
| DK=Don=t Know Where or Did not know about it | # |
Answer these insight questions below:
1. Rank order the 10 categories above according to the number of items listed in each one. Put the categories with the most items in it first, the second most second, and so on.
Most common is #1.
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|
2. After looking at the order of the origins of your sexual knowledge, consider the impact these origins have had on your sexual experience. Would you change their order? If so, why?
3a. Go back to the 40 items. Pick the top 10 which you believe to be the most significant. List their item numbers in the top row of boxes below.
Your top 10 Origin Code
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|
3b. Now take your top 10 picks and locate them on the origin boxes. Put the origin code below the item in the bottom row. Where did the most significant sexual knowledge originate for you? Would you change it if you could? Why, why not? Numerous studies of sexual learning indicate that most men and women learn about sex outside the home. How will you talk to your children about sex? Will you approach it the same way your parents did? Why, why not?
© 2014 Ron J. Hammond all rights reservedTelevision Messages about Sexuality
Many studies have established the fact that television viewing shapes our attitudes and outlook on life. This project is designed to facilitate an understanding of the sexual messages you get from various television shows. Watch two separate shows from 7-11:00PM and use this table to analyze their presentation of sexuality and sexual issues.
| Factors to Consider | First Show | Second Show |
|---|---|---|
| Title of the show | ||
| Actual count of sexual comments or innuendos? | ||
| Actual count of sexual acts or acts leading up to sex? | ||
| How many sexual jokes? | ||
| Was sex presented in a relational or non-relational context? | ||
| Was there any discussion of pregnancy or STD prevention? | ||
| How were sexual scripts & male and female stereotypes presented? | ||
| Were both partners equally interested and involved? How? | ||
| Would you feel comfortable knowing a 10 year old might be watching these shows? Why/why not? | ||
| Were biased racial & ethnic stereotypes reinforced? How? | ||
| Actual count of sexual messages in commercials: | ||
| Do these TV messages about sexuality reflect your own values? Why/ why not? | ||
| What was the purpose of sex in the plot of the show? | ||
| Was sex shown as an activity done with alcohol, drug, or other substances? | ||
| Was sex obtained through the use of violence? | ||
| Overall what percentage of the show had sexual themes? |
Additional Reading
Search the keywords and names in your Internet browser
Sexuality Information and Education Council of the United States has various reports and educational programs: SOURCE
US Center for Disease Control’s page on sexual health SOURCE
New York Online Access to Health in English and Español SOURCE
Kinsey Institute in Sex, gender, and Reproduction SOURCE
US Dept. of Health and Human Services site for women’s health SOURCE
Site for men’s health SOURCE
vast array of sex and other related health articles SOURCE
Just one more note: Sexual violence does not belong in a sexuality chapter of a textbook like this. It more appropriately belongs in a social problems, Intro to Sociology, Gender, or social deviance book. There is a free chapter on the issues of rape at http://freesociologybooks.com/ Introduction to Sociology Chapter 20 Rape and Sexual Assault